To learn more about our services and what we can do for you, or to make an appointment, call us today!
Snoring and Obstructive Sleep Apnea (OSA)
 Obstructive Sleep Apnea is a relatively new disease and, because of this, patients are cautioned to be informed consumers. OSA is a five-billion dollar industry, and as with all new and lucrative diseases, diagnosis and treatment are less constrained by knowledge. Issues to be aware of include the following:
Obstructive Sleep Apnea is a relatively new disease and, because of this, patients are cautioned to be informed consumers. OSA is a five-billion dollar industry, and as with all new and lucrative diseases, diagnosis and treatment are less constrained by knowledge. Issues to be aware of include the following:
- Exaggeration of the problem’s significance, hence, overdiagnosis and overtreatment are likely until the disorder is in reliable perspective.
- Management strategies are primitive and critical cost-benefit constraints are essentially absent.
- The diagnosis of OSA is made based on data obtained after one night in a sleep lab, which is unreliable because of the myriad of accommodation issues encountered by patients to a new environment and to their connections to monitors. This makes getting representative sleep very difficult. However, the sleep recordings are now being made at home for most patients and the data collected is more trustworthy.
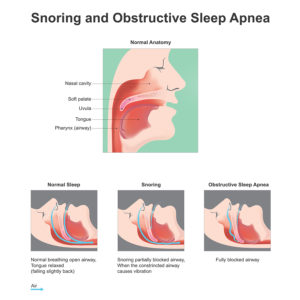
The relationship of snoring and OSA is that everyone who has OSA snores, but not everyone that snores has OSA. OSA occurs when snoring occludes the airway enough to cause a clinically relevant drop in blood oxygenation. The estimated prevalence of snoring is 40%, compared to a 17 % prevalence of OSA in adult populations. Snoring in the absence of OSA presents no known harm to the snorer, but commonly causes insomnia in bed partners. The same appliance used to treat OSA can be used to successfully manage snoring.
OSA refers to the partial or complete obstruction of one's airway during sleep. Partial obstruction is referred to as hypopnea, in which oxygen flow is diminished by at least 30% and blood oxygenation decreased by at least 4%. Apnea refers to complete obstruction of at least a 10 second duration. The frequencies of hypopnea and apnea events determine indices used to classify OSA. These indices are AHI (Apnea-Hypopnea Index) and RDI (Respiratory Disturbance Index). The classifications are as follows:
- Normal: less than 5 events per hour
- Mild: 5 to 15 events per hour
- Moderate: 15 to 30 events per hour
- Severe: more than 30 events per hour
OSA symptoms include snoring, gasping for breath during sleep, excessive daytime sleepiness, and insomnia.
- Risk factors for OSA include obesity, nasal congestion, alcohol ingestion before bedtime, smoking, and a retruded lower jaw.
- Men are twice as likely as premenopausal women to suffer from OSA, but this male predilection disappears in women following menopause.
- Co-existing diseases that may be related to OSA include cardiovascular disease, GERD (gastro-esophageal reflux disease), obesity, depression, impotence, glucose intolerance, and bruxism. The most common cause of airway obstruction is the tongue, although nasal passage obstructions and allergies are relevant.
The diagnosis of OSA can be made based on clinical symptoms, home sleep testing, and sleep lab testing (polysomnography). Imaging is generally not helpful and polysomnography is the “gold standard”. However, the correlation between OSA clinical symptoms and home testing are reliable. Generally, polysomnography is required for insurance carriers to provide treatment coverage, and only physicians are allowed to make the diagnosis. The approximate cost of a sleep lab diagnosis is between $1,200 and $2,400.
The treatments for OSA include CPAP (Continuous Positive Airway Pressure), Mandibular Advancement Devices (MADs), and Surgeries. The goal of treatment is to reduce the AHI/RDI to less than five events per hour.

- CPAP involves the forcing of air through the nostrils and requires a mask and pressurizing device.
- CPAP is slightly more effective than MADs for the treatment of severe sleep apnea.
- Drawbacks to CPAP include poor portability, increased expense, problems adjusting to the mask, air leakage, noise, and the restriction of a patient's sleep position.
- Patient compliance with CPAP is only approximately 50%.
- Compared to a MAD, CPAP is less user-friendly and has poorer patient compliance.
- MADs are removable oral appliances attached to both the upper and lower teeth, holding the lower jaw forward, which brings the tongue forward and opens the airway. Once the airway is open, it does not matter whether the patient breathes through their mouth or their nose.
- Patient compliance rate with MADs is approximately 90%, much higher than CPAP.
- MADs are just as effective as CPAP for the treatment of mild and moderate OSA and are slightly less effective with severe sleep apnea.
- The advantages of MADs compared to CPAP include portability, less expense, and improved patient compliance.
- Drawbacks to MADs can include the worsening or development of TMD signs and symptoms and permanent changes in one's bite (occlusion). However, for most patients, MADs improve TMD symptoms and are recommended for patients with both OSA and TMD. If TMD symptoms develop, they are usually mild and easily managed. Bite changes are also uncommon and when they do occur, patients will be aware of them in time to stop wearing the appliance and, thereby, avoid permanent bite changes.
- With MADs, the further forward the mandible is positioned, the more you open the airway and the greater the impact on OSA. However, the likelihood of jaw pain increases as the mandible is advanced.
- There are appliances that just hold the tongue forward (Tongue Retaining Devices), however, these appliances are less effective than MADs.
- CPAP and MADs can be used in combination simultaneously or MADs can be utilized for travel by patients who use a CPAP at home.
- Treatment success can be gauged by the improvement in clinical signs and symptoms and repeat polysomnography.
- Given the improvement in patient compliance and the equal efficacy in the treatment of mild and moderate OSA, one might expect physicians to refer appropriate patients for MAD therapy. However, physicians usually refer all patients for CPAP and will only refer patients for MADs if the patient refuses to use CPAP or cannot tolerate it.
- Because of the strong correlation between weight and OSA, weight loss can be a permanent cure for OSA.
- In the absence of a clear pathology, surgery is considered only after more conservative measures have been attempted and failed. Surgeries may include:

- Partial removal of soft palate and tongue tissues
- Removing tonsils and adenoids
- Advancing the tongue or the mandible
- Surgically opening nasal and sinus airway passages
Treatment Concerns
Upper Airway Resistance Syndrome (UARS) refers to a proposed designation of airway pathology that is more subtle than OSA, and hence, can make airway disease more ubiquitous and more responsible for relatable problems. At this time, UARS lacks acceptable scientific validation and is of questionable merit.
Currently, there are practitioners who claim that all nocturnal bruxism is caused by OSA/UARS and that OSA/UARS is responsible for all TMD problems. Such assertions not only lack scientific validation but are at odds with both present scientific findings and clinical practice. It is highly improbable that such sweeping correlations are true and consumers should be cautious if confronted by such assertions.
Similarly, OSA is a relatively new, and hence, topical disorder. Past history has shown that such “hot topics” are usually overdiagnosed and overtreated until longitudinal research can put their prevalence and need for treatment in perspective. For example, the long-term impact of OSA on one's general health and longevity is unclear.
Sleep Hygiene Tips
Changing certain bedtime habits may result in better sleep. While these changes may take time and effort, the improvement is worth it.
- Sleep on your side. If you sleep on your back, gravity may pull the tissues of your throat down and your tongue back, blocking the airway. Sleeping on your side may help keep the airway open.
- Lose weight. Folks who are overweight often have excess bulky tissues in their throat which can make snoring and apnea worse. Your physician can help you develop a plan to lose weight and keep it off.
- Exercise. Exercising is recommended but should be avoided within 3-4 hours of bedtime as the increase in adrenalin can impair sleep.
- Avoid alcohol and certain medications. Alcohol and some medications, like sleeping pills, some antihistamines, and sedatives, can relax the muscles of your throat, which may worsen snoring and apnea. Avoiding alcohol 3-4 hours before sleep is recommended. Talk to your doctor about medications you take that may impact snoring and apnea.
- Clear your nose. A clogged nose does not let air in as easily. Allergies and sinus problems can also contribute to difficulty breathing through your nose. Nasal strips, rinses, and sprays can help make breathing easier. Your doctor can recommend these if they are appropriate.
- Don't eat near bedtime. Allow 3-4 hours between eating and bedtime.
Our Mandibular Advancement Devices (MADs)

- MADs are available in many designs, though they all attempt to accomplish the same end result.
- Our MAD is fabricated by a laboratory and is made of processed acrylic with ball clasps for retention. This device is well tolerated and extremely durable. (Photos above and to the right)
- Patients cannot adjust the appliance, but the position can be changed by Dr. Montgomery.
- We commonly give patients a hypnotic agent to assist sleep during the accommodation period. It is important to understand that the appliance, like CPAP, can only be effective if utilized by patients. If patients have difficulty adjusting to the MAD, trouble sleeping or pull the device out during sleep, the treatment will fail. The only means to avert these problems is to obtund consciousness by having these patients take a hypnotic agent at bedtime. Not all patients need this, but some need the medication only while getting used to the appliance, while other patients need the medication long-term. Because the airway is being held open by the MAD, the potential negative effects of the hypnotic agent are neutralized.
Our Treatment Protocol
- First Appointment: Approximately 1 hour
- Clinical examination
- Screening jaw image
- Discussion of the problem and treatment options
- Impressions for the appliance, if indicated. The appliance requires approximately one week for fabrication by our laboratory.
- Second Appointment: Approximately 30 minutes
- Delivery of the appliance
- Prescription of a hypnotic agent, if desired/needed
- Follow-Up Appointments: Approximately 30 minutes each
- Generally, 1-3 appointments separated by two weeks
- The number of appointments needed depends on the problems encountered and the efficiency of success.